


Seraccess® Automated Glucose Monitoring (AGM) for Hospital Care
Seraccess® AGM - Automated and regular glucose measurement for the monitoring, detection and treatment of dysglycemia.
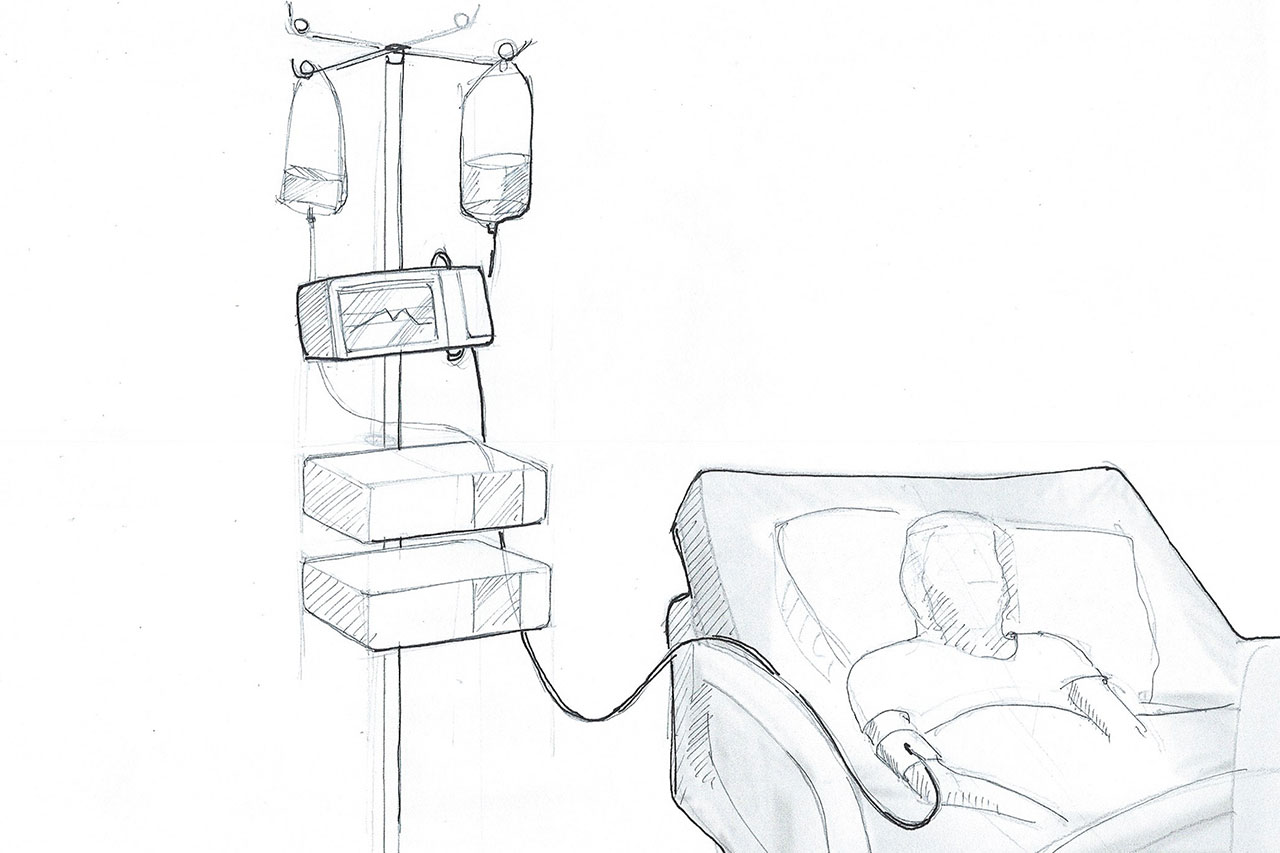
Seraccess® AGM is a system that revolutionizes the way disglycemia is treated today in the hospital, and especially in the intensive care unit (ICU). Avoiding dysglycemia is a key goal in the treatment of patients in ICU.1-5 Unfortunately, both hyper- and hypoglycemia in hospitals are common and related to increased morbidity, mortality, and respectively increased health care costs.6 Automated glucose measurement reduces resource utilization and nursing costs, as well as length of stay in the ICU by more than a day.5,7,8 Seraccess® AGM is a system that can be integrated in existing installations to provide optimum glucose monitoring.
Why Seraccess® AGM?
Current glucose measurement methods are mainly based on manually drawn blood samples. There are often large time intervals between measurements, and the total time needed by the nursing personnel generates significant cost. Seraccess® AGM performs automated and regular blood sampling, using an already inserted catheter. Only a tiny amount of blood is required for each measurement and the system provides highly accurate and precise glucose values at short time intervals. Seraccess® AGM enables physicians to follow a patient's course of blood glucose in a much closer way and empowers confident treatment decisions.
The Seraccess® AGM Approach
The automated, regular, accurate and precise glucose measurement provided by Seraccess® AGM will empower confident treatment decisions and can lead to improved clinical outcomes. Furthermore, hospitals benefit from significant cost reduction by eliminating manual glucose measurements.
How much blood is needed per day to measure blood glucose every 15 minutes?
The Seraccess® technology only needs 20µl to 30µl of blood to perform a measurement. At a frequency of 15 minutes, this results in 96 measurements per day which amounts to just 2ml to 3ml of blood needed per day.
Opportunity
Over 200,000 beds in intensive care units in the US and Europe alone translate to a yearly potential of at least 35 million treatment days generated by about 9 million patients. An ICU bed equipped with the Seraccess® AGM durable unit will host around 100 patients per year, who will consume 200 disposable units. Overall, the value of the durable market is estimated at 1.4 bn CHF and the disposable market at 2.7 bn CHF.
Milestones
The benefits of the intravenous pathway - Part III
How does the Seraccess® blood glucose measurement perform in healthy subjects when compared to Cobas C111?
Learn moreThe benefits of the intravenous pathway - Part IV
How does the Seraccess® blood glucose measurement compare to state-of-the-art CGM?
The benefits of the intravenous pathway - Part V
How does the Seraccess® blood glucose measurement perform in healthy subjects when compared to YSI?
Learn moreThe quality of Seraccess®’ continuous automated blood sampling via an existing catheter. Part I
Does Seraccess®'s automatic blood sampling, including sample preparation using the silicon membrane developed and patented by Securecell, work in vitro in a regulated blood circuit?
Learn moreThe benefits of the intravenous pathway - Part VI
How does the Seraccess® blood glucose measurement perform in subjects with type 1 diabetes when compared to Cobas C111?
Learn moreThe quality of Seraccess®’ continuous automated blood sampling via an existing catheter. Part II
Does Seraccess®'s continuous automatic blood sampling work in vivo on live sheep?
Learn moreSeraccess® is a mid-stage venture project of Securecell that offers investment opportunities to private and institutional investors.
All information and opinions contained herein have been prepared by management and its advisors and represent their assessment as of January 2022. No representation or warranty, expressed or implied, is given as to the accuracy or completeness of the contents, opinions, or projections expressed herein and no responsibility or liability is accepted. All information videos and contents do not constitute an offer to purchase securities. The website content does not constitute an invitation to buy shares under US or international law.
References:
1 I.B. Hirsch, L.M. Gaudiani: A new look at brittle diabetes. Journal of Diabetes and Its Complications 35 (2021) 107646; https://doi.org/10.1016/j.jdiacomp.2020.107646
2 Cryer, P.E., S.N. Davis, and H. Shamoon, Hypoglycemia in diabetes. Diabetes Care, 2003. 26(6): p. 1902-12.
3 Lind, M., et al., Glycemic control and excess mortality in type 1 diabetes. N Engl J Med, 2014. 371(21): p. 1972-82.
4 Cartwright A. et al. The outcome of brittle type 1 diabetes - a 20 year study. Q J Med 2011; 104:575-579
5 Flanagan D. What happens to people with “brittle” diabetes? Diabetes Digest 2011 Vol 10;4:196 https://www.pcdsociety.org/download/resource/2756; accessed Dec 16, 2021
6 https://www.webmd.com/diabetes/brittle-diabetes-all-about; accessed Dec 15, 2021
7 CDC National Diabetes Statistics Report 2020; https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf; accessed Dec 15, 2021
8 https://www.americanactionforum.org/research/understanding-the-insulin-market/; accessed Dec 15, 2021
9 https://www.bdtype1.com/difference-stable-type-1-vs-brittle, accessed Dec 20, 2021
10 Lyerla et al. Recurrent DKA results in high societal costs - a retrospective study identifying social predictors of recurrence for potential future intervention. Clin Diabetes Endocrinol (2021) 7:13; https://clindiabetesendo.biomedcentral.com/track/pdf/10.1186/s40842-021-00127-6.pdf
Be up to date
Subscribe to our exciting newsletter and don't miss any information. It's worth it!